OpenAge.
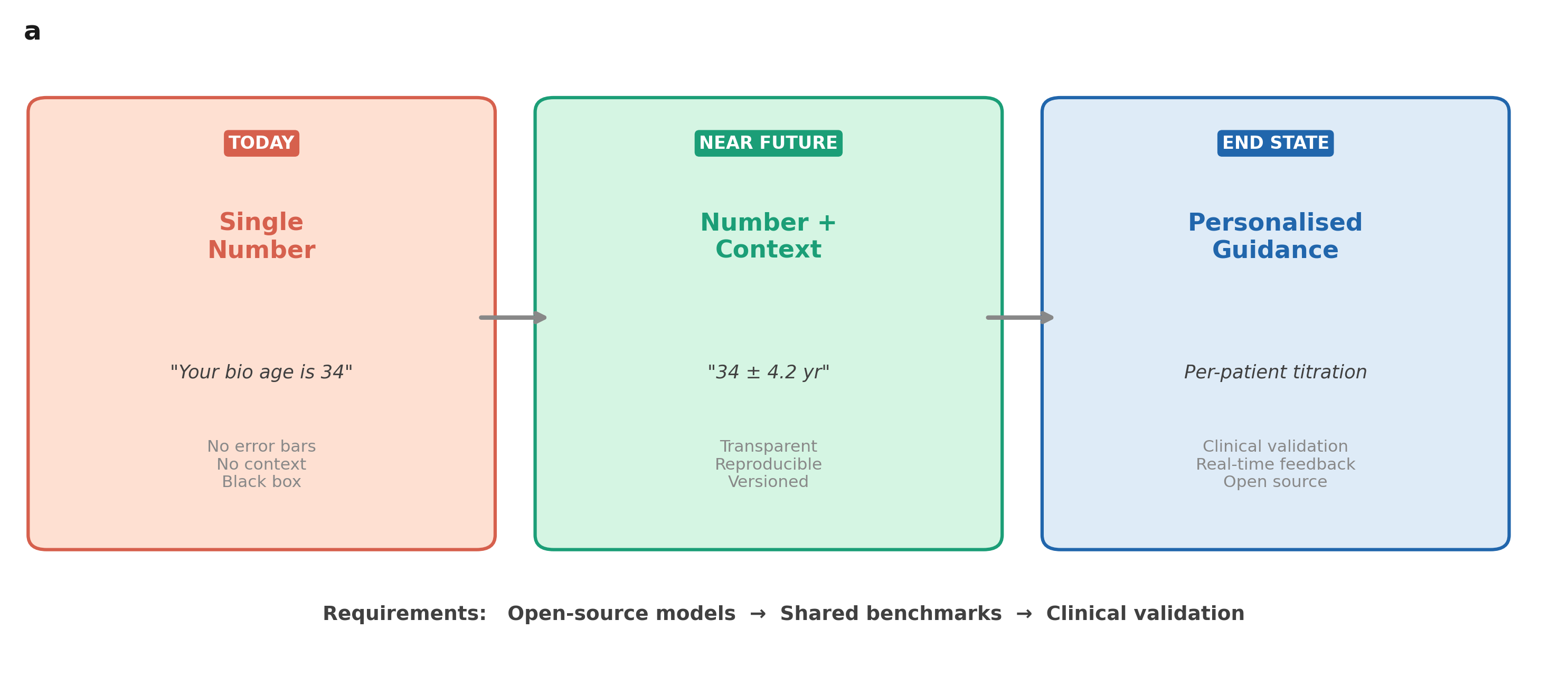
An open-weight
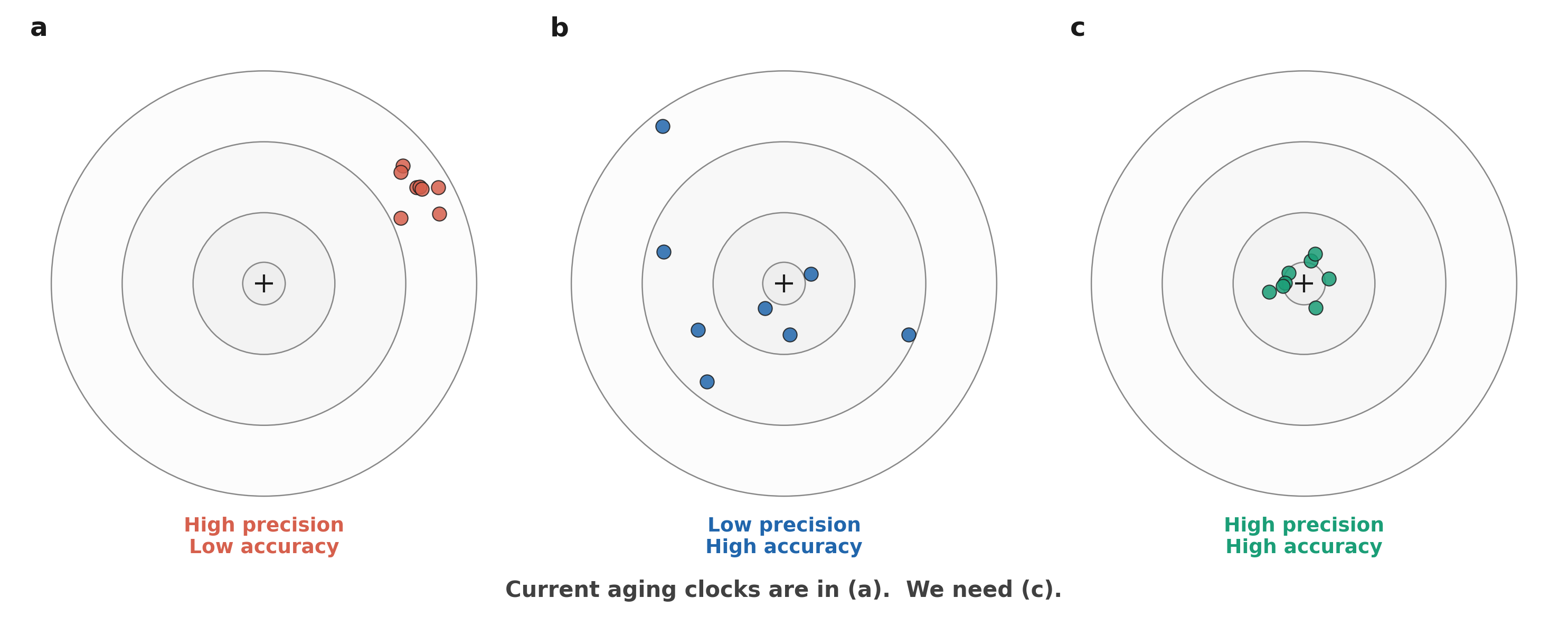
biological aging clock
validated against
actual death.
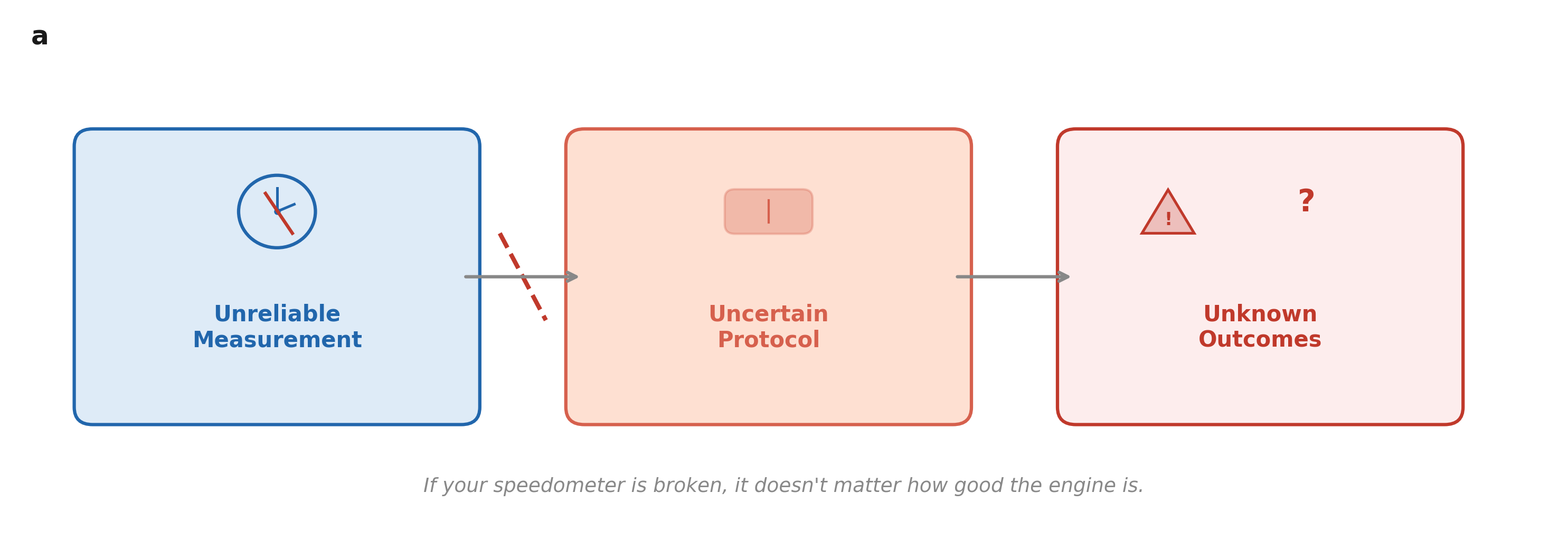
"You can't run ML benchmarks
on most of biology.
You can on aging."
on most of biology.
You can on aging."
Nikhil Yadala · Healome One Inc.
github.com/Healome/OpenAge · OpenAgeAI.com
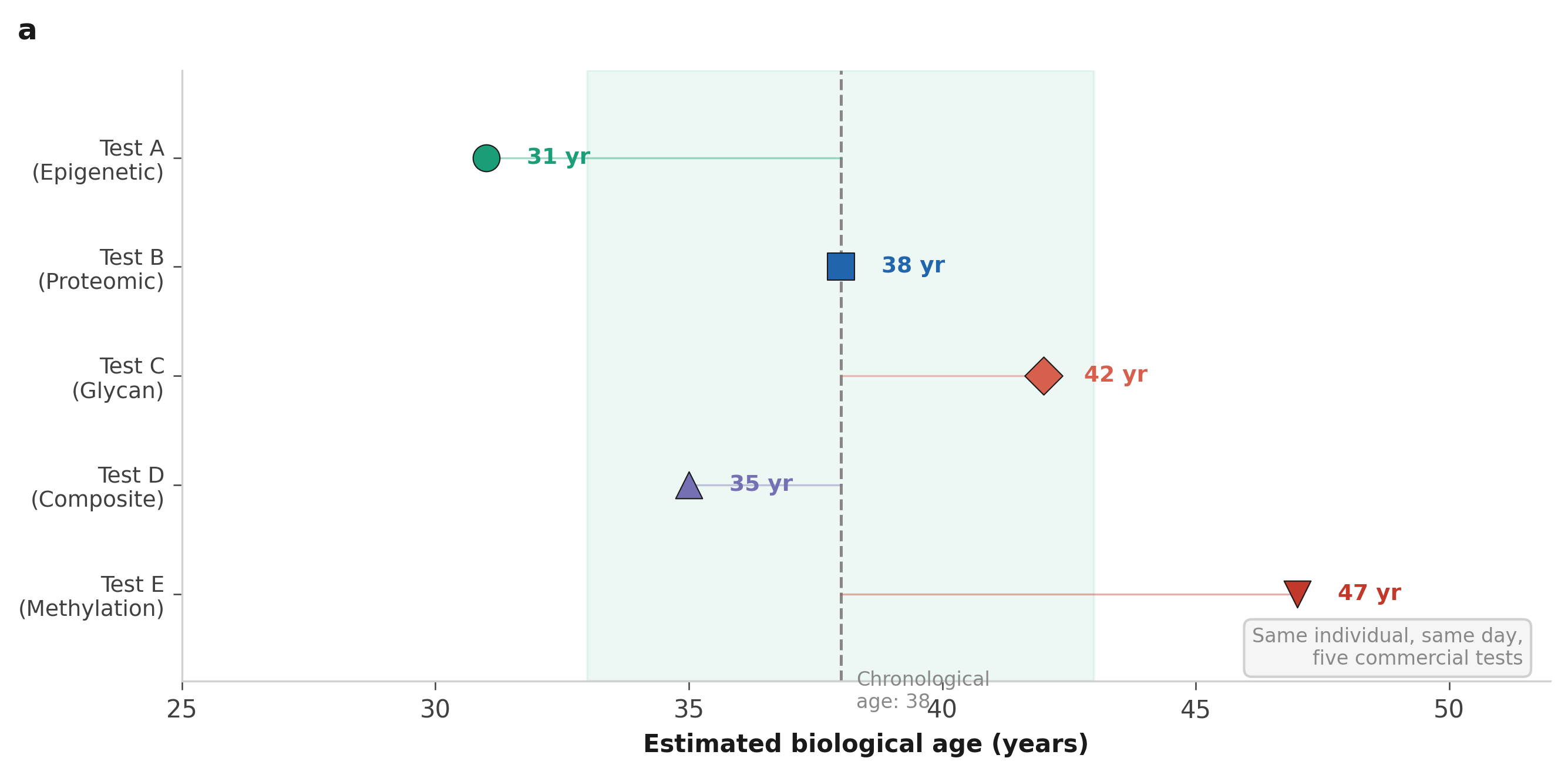
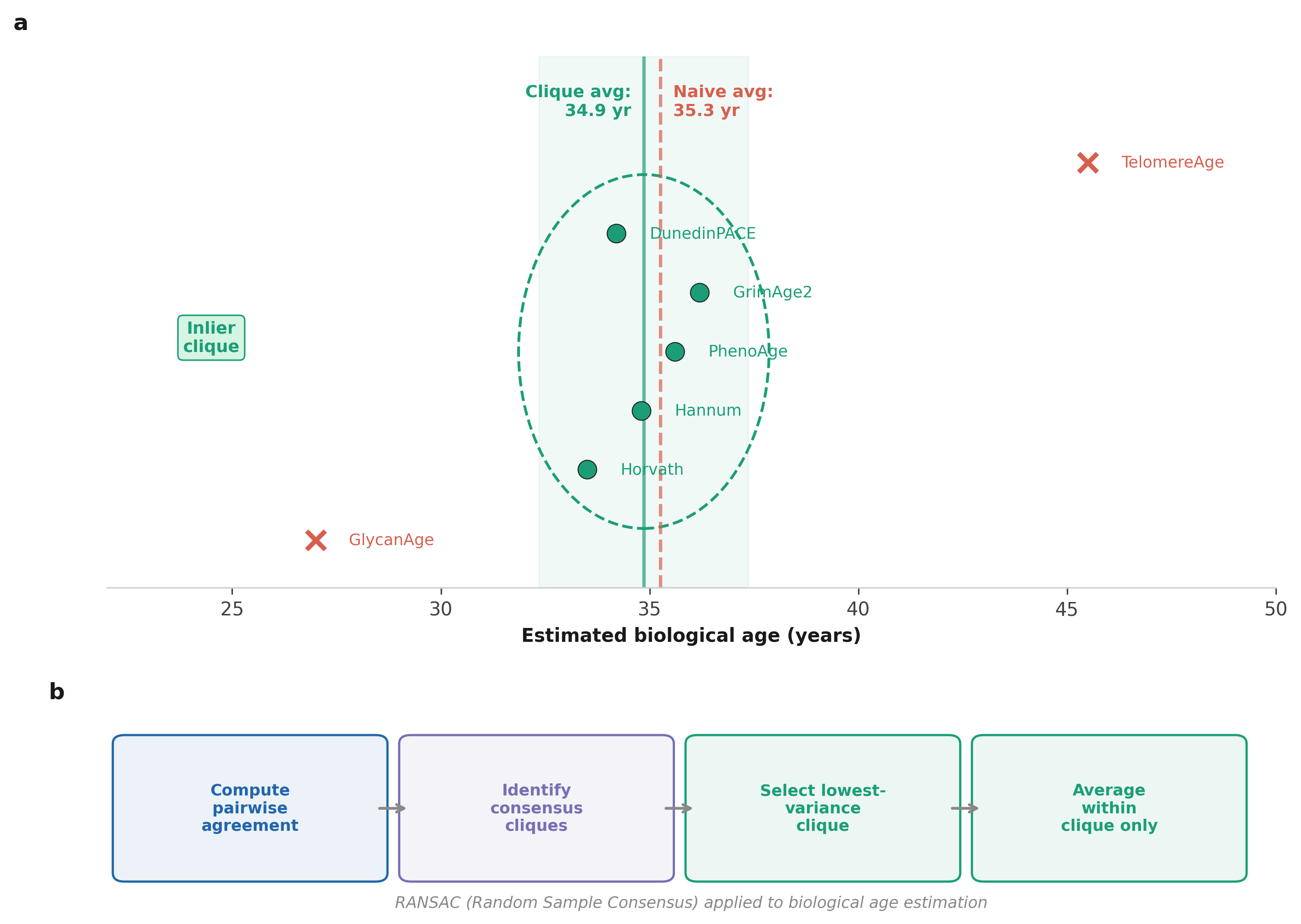
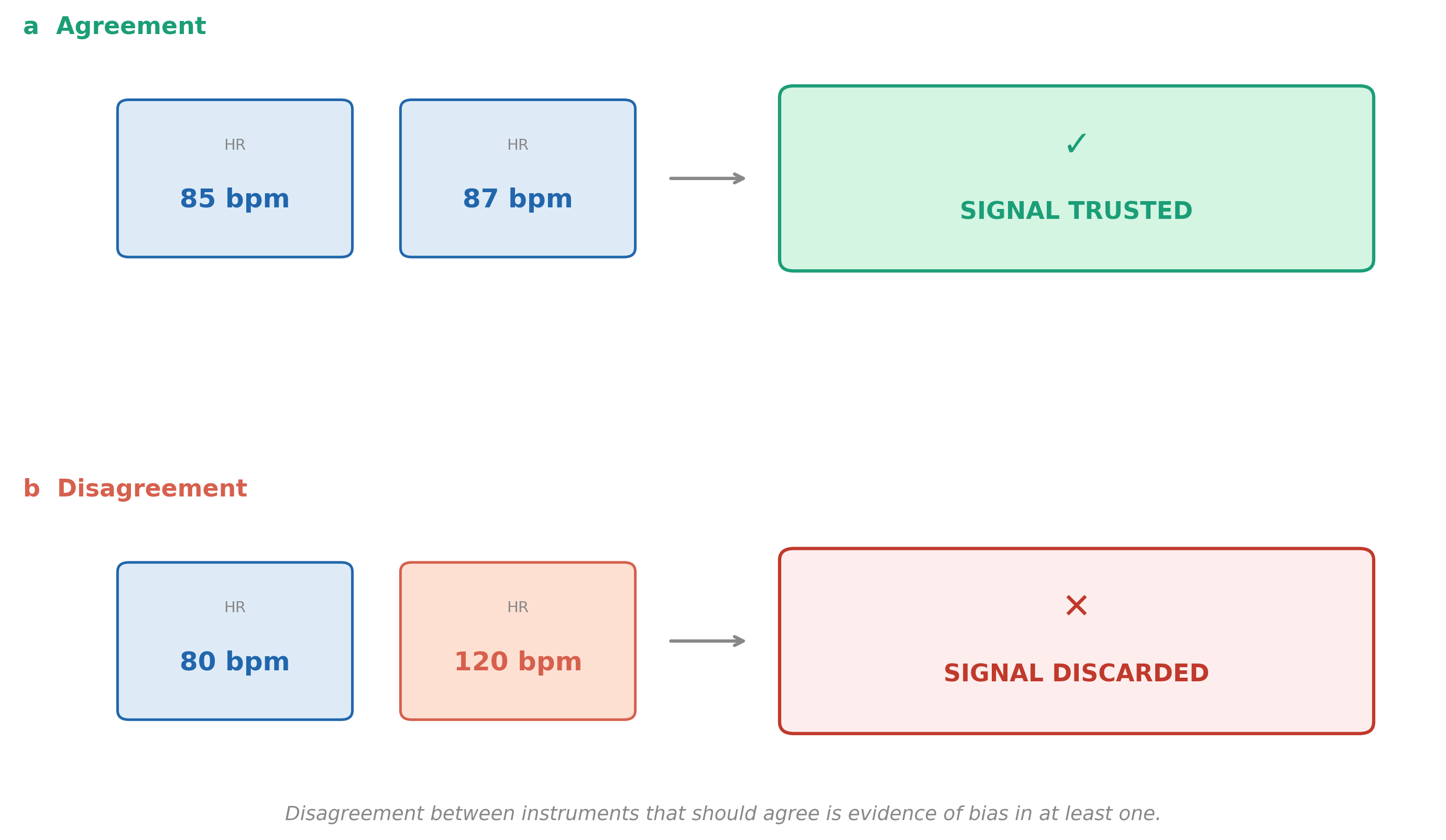
Different tests. Different answers.
OpenAgeAI.com